



This summary covers:
- Prediction and Prevention of Spontaneous Preterm Birth - Practice Bulletin #234 - Published August 2021
- Management of Preterm Labor - Practice Bulletin #171 - Published October 2016
Prediction and Prevention
Five Pearls
PTD at <34 wga carries higher mortality and morbidity risk to newborn in delivery and long-term morbidity
History of PTD is the greatest risk factor for PTD in a current pregnancy
Progesterone supplementation can be considered regardless of history of PTD
In patients w/ singleton pregnancy and history of PTD, cerclage should be offered if CL <25 mm is detected on TVUS at 16-24 wga
Omega 3s, low-dose aspirin, lifestyle modification, and smoking cessation are also important considerations in decreasing our national PTD rate
Background
rates of preterm delivery in the U.S. has been pretty stable
"Although risks are greatest for neonates born before 34 weeks of gestation, infants born after 34 weeks of gestation but before 37 weeks of gestation are still more likely to experience delivery complications, long-term impairment, and early death than those born later in pregnancy"
risk factors for PTD: prior PTD (1-2x ↑ risk), short cervical length (<20mm if no history of PTD; <25mm if prior history), vaginal infection in pregnancy, vaginal bleeding in pregnancy, UTI in pregnancy, or periodontal disease in pregnancy (treatment of any of these won't normalize risk, though), low maternal BMI, smoking, substance abuse, and short inter-pregnancy interval
in case you were wondering, history of LEEP of CKC for cervical dysplasia has not been found to be a risk factor after all according to ACOG but there are studies that support this (and my own direct clinical experience reflects the alternative)
White women have the lowest rate (9.3%), Hispanic women (10%), American Indian and Alaskan native (11.5%), Native Hawaiian and Pacific Islander (11.8%), with highest rates seen among black women (14%)
Who should be screened and how?
the purpose of screening is to identify patients in whom intervention will be helpful
really the only patients who qualify for screening are those with a history of prior PTD, PPROM, multiple gestations, but ACOG feels it’s reasonable to screen universally as 5% of all women could potentially give birth preterm
a systematic review looked at 14 studies and found that:
“a cervical length less than 25 mm before 16-24 weeks of gestation had a sensitivity of 65.4% for preterm birth before 35 weeks of gestation, with a positive predictive value of 33.0% and a negative predictive value of 92.0%. Sub-analysis of the studies that included only women whose risk factor was prior spontaneous preterm birth found a similar sensitivity and a positive predictive value of 41.4%”
get a baseline transvaginal ultrasound (TVUS) and repeat this evaluation every 1-2 weeks to assess for change (limited data on time interval)
measure three times, and go with the average
"fetal fibronectin screening, bacterial vaginosis screening, and home uterine activity monitoring have been proposed to assess a woman’s risk of preterm delivery" and none of them have panned out as useful predictors of PTD in asymptomatic women
recent data suggests that it might actually be cost-effective to universally screen for shortened cervix in patients without history of PTD (study 1, study 2), but, for now, ACOG states it's reasonable to offer but not necessarily recommended universally

When and how to prevent PTD?

No history of PTD
Extensively studied as a means to reduce the risk of preterm birth in asymptomatic women with a singleton pregnancy, short cervix, and no prior preterm birth.
a meta-analysis of five randomized trials of vaginal progesterone versus placebo in patients with a singleton pregnancy, a short cervix, and no prior preterm birth was performed, including patients from the 2019 OPTIMUM (Does Progesterone Prophylaxis to Prevent Preterm Labour Improve Outcome?) trial who did not have other risk factors, and standardizing the threshold definition of shortened cervix at 25 mm or less for their analysis. Patients treated with vaginal progesterone had a significantly reduced risk of any preterm birth before 34 0/7 weeks of gestation (14.5% versus 24.6%; RR, 0.60; 95% CI, 0.44–0.82), spontaneous preterm birth before 34 0/7 weeks of gestation (RR, 0.63; 95% CI, 0.44–0.88), neonatal respiratory distress, and neonatal intensive care unit admission. The meta-analysis authors calculated that 14 patients would need to be treated to prevent one spontaneous preterm birth before 34 0/7 weeks of gestation.
Vaginal progesterone is recommended for asymptomatic individuals without a history of preterm birth with a singleton pregnancy and a short cervix. 200 mg per vagina nightly is the best studied regimen
History of PTD:
Before the PROLONG trial (2020), a metaanalysis was published in 1990 that showed demonstrable evidence of the benefits of 17-OH-P in preventing recurrent PTD, which led to a large multicenter RCT of 463 patients. They were randomized to receive either 250 mg 17-OHPC IM or placebo, starting between 16 0/7 and 20 6/7 weeks of gestation. Administration of 17-OHPC reduced the rate of preterm birth before 35 weeks of gestation by one third, leading ACOG and SMFM to recommend this intervention universally to women with history of PTD.
Then came the PROLONG trial, which evaluated the efficacy of 17-OHPC 250 mg intramuscular injection weekly compared with placebo on preterm birth and neonatal morbidity among women with a singleton pregnancy and prior spontaneous preterm birth. Large, international, multicenter double-blind RCT. 1740 women randomized (of 1877 eligible). No statistical difference found in the two primary outcomes of preterm birth before 35 0/7 weeks of gestation or maternal/neonatal outcomes.
On April 5, 2023, the FDA withdrew its approval of 17-OHP for prevention of preterm birth as a result of the PROLONG trial
Data comparing vaginal to IM progesterone supplementation continues to roll in, so no definitive conclusions can be made yet
In the meantime, SMFM discourages clinicians from using IM 17-OHP off-label
Recommended to screen cervical length every week from 16-24 weeks and to offer cerclage if it measures <25 mm, though this intervention was best studied for women with history of PTD <34 weeks
it may be more cost effective to forego cervical shortening screening altogether in those without this history
Cerclage
Short cervix found on ultrasound: uncertain effectiveness in patients with a short cervix and no history of preterm birth. However, there is evidence of potential benefit in patients with a very short cervical length (<10 mm)
Open cervix on physical exam: Individuals with cervical insufficiency based on a dilated cervix on a digital or speculum examination at 16 0/7–23 6/7 weeks of gestation are candidates for a physical examination-indicated cerclage (but data is mixed)
unclear if 17-OH-P plus cerclage are additionally helpful together compared to either intervention alone
An interesting side note: there’s no evidence, per say, that suggests that it’s a terrible idea to place an US-indicated cerclage after 23 6/7 weeks; this is merely “expert opinion”
Because cervical insufficiency traditionally is defined as painless cervical dilation in the 2nd trimester, this restriction presented no issue when viability did not begin until the 3rd trimester and indeed may have arisen to discourage the treatment of patients with threatened preterm labor with cerclage
But now that we have better means of keeping 23+ weekers alive in the NICU, it seems that little investment has been made to prevent babies from coming super early
What if a specific institution doesn’t have the full capacities for keeping these very preterm babies alive? Should we not then consider an early 3rd trimester cerclage? Why not? Very little data to continue this conversation…(much of this is paraphrased from a bada$$ article that was recently published in the Green Journal)
Notes on cerclages...
There are three indications:
Ultrasound-indicated: what we've already described
History-indicated: cerclage placed at conclusion of first trimester and after prenatal screening has been completed in patients with cervical insufficiency
Physical exam-indicated (e.g. rescue cerclage): option if cervical dilation >2cm is visualized on speculum exam or ultrasound <24 wga
There are three techniques (all call for Mersilene suture):
McDonald: performed vaginally under regional anesthesia using the purse-string technique at the cervicovaginal junction; bladder emptying is recommended, but mobilization is not required
Shirodkar: performed vaginally under regional anesthesia using purse string technique after emptying and mobilizing the bladder
Transabdominal: performed laparoscopically or open, placing the suture in purse-string fashion at the cervicoisthmic jxn (**will require c-section); recommended if vaginal placement is determined not possible or if cervix is too short that vaginal effort is unlikely to be successful
If a patient has a cerclage in place and presents in active labor, you must remove the cerclage to avoid cervical laceration, which can lead to outrageous brisk bleeding (you can't stop active labor)
Other options
if birth was preterm due to other comorbidities, low-dose aspirin has been demonstrated in some studies to prevent preclampsia and thus prevent indication for iatrogenic preterm birth
tighter control over BPs in cHTN may also decrease our PTD rates
presence of funneling hasn't been found to significantly influence the risk of PTD
"indomethacin or antibiotics, activity restriction, or supplementation with omega-3 fatty acids have not been evaluated in the context of randomized trials for women with short cervical length, and are not recommended as clinical interventions for women with an incidentally diagnosed short cervical length."
stop smoking
omega 3 fatty acids show some promise (2018 Cochrane review)
decreasing allostatic load (think: improve our racist, inegalitarian society)
treat UTIs and vaginal infections when they arise
false unicorn root
wild yam
uva ursi (indirectly through flushing urinary tract)
history of PROM: check electrolytes or hair mineral analysis
Management of Preterm Labor
Five Pearls
Preterm labor carries significant risks to the newborn: the more premature, the worse the outcomes
Given high risk for long-term morbidity in extremely premature infants, focusing on comfort as opposed to aggressive resuscitation at time of delivery is reasonable through a shared medical decision-making process
Corticosteroids can improve outcomes for newborns at risk of preterm birth at <34 wga (and some as late as 36w5d) if delivery anticipated within the next 7 days
Latency antibiotics can improve outcomes for newborns in the setting of PPROM at <34 wga
Magnesium sulfate can improve outcomes for newborns at risk of preterm birth at <32 wga
Background
around 10% of babies are born before 37 wga
why are we concerned? higher risk of neonatal mortality, respiratory distress, sepsis, intracranial bleeding, and long-term issues like neurodevelopmental challenges
preterm labor definition: regular uterine contractions + cervical dilation ≥ 2 cm between 20 wga and 36w6d ga
<10% of women who present that meet these criteria actually deliver within 7 days
So a patient presents with contractions preterm...
you could look with a speculum exam, collect fetal fibronectin, and/or get an endovaginal ultrasound
utility of ultrasound and FFN haven't been validated through RCTs, though observational data suggests they may be helpful in identifying patients truly at risk for preterm birth; FFN alone has poor predictive value (CONSIDER THE WHOLE CLINICAL PICTURE)
if she looks like she's in labor, especially if >32 wga, digital exam of the cervix may be warranted - we will review prevention of preterm labor in a future episode...
When should we be worried about preterm delivery?
consistent regular contractions and evidence of cervical dilation are good sign that preterm delivery may be happening
in 30% of patients presenting w/ preterm prodromal labor, the process will cease spontaneously; only 50% of patients admitted for preterm labor concerns will end up delivering at term (SO BE JUDICIOUS AND THOUGHTFUL)
Pearl: ~20% of patients who present with preterm contractions without cervical dilation will deliver before 37 wga; <5% will deliver within 2 weeks of presentation
Can we stop preterm labor?
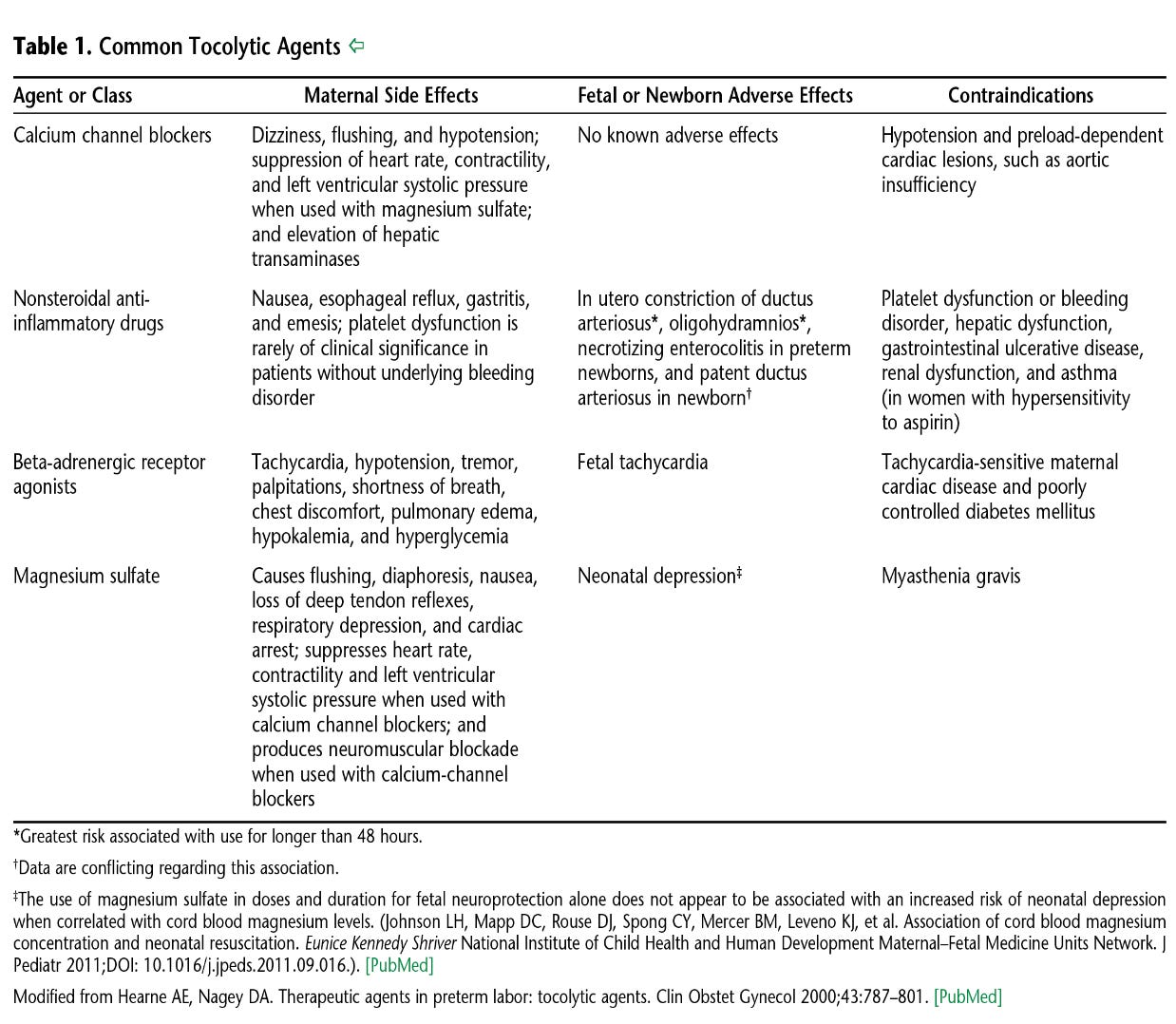
Sometimes, but tocolytic therapy is only thought to be effective for 48 hrs (just so happens to buy you enough time to get corticosteroids on board if indicated)
tocolysis is generally not recommended after 34 wga
since 30% of preterm labor will resolve without any intervention, even patients with advanced cervical dilation (2 cm) at <34 can generally be observed without tocolytics, and particularly so if no cervical dilation is found
b-adrenergics don't tocolyze well and carry significant maternal cardiovascular risks (but OK for antepartum uterine tachysystole)

What's the cut off for viability?
<20 weeks is considered previable (no intervention indicated)
23 wga to ~26 wga can be considered periviable
this NICHD calculator can be used in your counseling to guide delivery/management plan
Pearl: Just because we can resuscitate a baby doesn't mean that we should. Delivery of a peri-viable newborn must include risks and benefits of delivery methods to mom and risk and benefits of preterm delivery and resuscitation to the newborn.
What's the role of corticosteroids?
stimulates the development of alveoli in premature fetal lungs in order to optimize transition to external environment
can significantly improve outcomes
recommend a single course if patient presents with preterm labor (or need for delivery due to maternal health concerns like early-onset severe preeclampsia) between 23 wga and 33w6d if you anticipate delivery within 7 days
can repeat the course if greater than 2 weeks have passed after first course
can recommend single course between 34 wga and 36w5d if i) no prior steroids, ii) membranes intact, iii) patient not diabetic (and don't delay delivery to complete course)
Regimens:
a. betamethasone 12-mg IM q24 hrs for 2 doses
b. dexamethasone 6-mg IM q12 hrs for 4 doses
Should I mag or should i not?
if <32 wga, start mag for fetal neuroprotection
mag isn't a reliable tocolytic agent
if patient is on mag for fetal neuroprotection, adding on a tocolytic agent can still be considered, but be careful with b-agonists and Ca-channel blockers (synergistic w/ mag sulfate, so may cause hypotension); go with indomethacin
Should I recommend antibiotics?
intrauterine infection is a well known cause of preterm labor and delivery
antibiotics haven't been found to be helpful outside of PPROM at <34 wga ("latency" abx)
latency antibiotics have been found to improve interval from time of PPROM to delivery, ↓ risk of chorio, neonatal infection, and need for neonatal oxygen therapy (Cochrane Review) in patients who present w/ PPROM at <34 wga
The regimen:
2x days ampicillin 2 g IV q6hr PLUS erythromycin 250 mg IV q6hr THEN 5x days amoxicillin 250 mg PO q8hr PLUS erythromycin 333 mg PO q8hr
erythromycin and azithromycin are equally efficacious, but the latter is cheaper and better tolerated from GI standpoint
amoxicillin-clavulanic acid (augmentin) associated with higher risk of neonatal necrotizing enterocolitis (NEC) in some studies, therefore not recommended
If PCN allergic:
Azithromycin 1 g PO x1 at time of admission PLUS 2x days cefazolin 1g IV q8hr THEN 5x days cephalexin 500 mg PO four times daily
if severe PCN allergy, substitute cephalosporins for gentamicin/clindamycin
at 34 wga, it's prudent to recommend IOL (risks versus benefits)
What can be done to prevent preterm delivery?
hydration, bed rest, nor tocolytics in asymptomatic women have been found to be helpful prophylaxis against preterm delivery
plus there's potential harm from decreased activity: ↑ risk VTE, ↑ bone demineralization, and general de-conditioning
Atosiban is a maintenance tocolytic that isn't FDA approved for use in the US
What about preterm delivery in multiple gestations?
no clear data to support the benefit of steroids or mag sulfate for fetal neuroprotection in multiple gestations
many experts extrapolate that benefits outweighs risk, though
tocolytics: risks outweigh benefits in multiple gestations
Notes for this episode are found on Substack
Work with Nathan:
Beloved Holistics | Born Free Method | Clear & Free | Twins-Breech
Medical Disclaimer: Born Free Method: The Podcast is an educational program. No information conveyed through this podcast should be construed as medical advice. These conversations are available to the public for educational and entertainment purposes only.
Music provided by RealMovieScores / Pond5





Share this post